EII en niños. Correlación clínico-radiológica y estadificación del grado de actividad
Palabras clave:
poster, seram, niños, pediatría, EIIResumen
Objetivos
La EII se diagnostica en un 25-30% de los casos durante la infancia y adolescencia. Objetivos:
- Analizar la correlación entre los hallazgos radiológicos y los datos clínicos, analíticos, endoscópicos e histológicos.
- Valorar la concordancia entre la ecografía y la E-RM.
- Destacar los hallazgos de imagen más relevantes que ayuden a establecer el grado de actividad de la enfermedad.
- Valorar el papel de las técnicas de imagen (ecografía, E-TC y E-RM) en el diagnóstico y seguimiento de la EII en los niños.
Material y métodos
Hemos revisado las historias de 40 pacientes con sospecha clínica de EII desde octubre de 2010 hasta septiembre de 2015. A todos se les realizó ecografía y a 38 entero-RM. 15 pacientes fueron diagnosticados de EC y 10 de CU. A 23 de los 25 pacientes den EII se les realizó entero-RM. A los otros dos pacientes con EII se les realizó TC (un lactante con EC y una niña de 12 años con CU complicada con megacolon tóxico).
Se ha utilizado un ecógrafo Siemens Acuson Antares, con sonda convex de 3-5 MHz y sonda lineal de alta frecuencia (7-10 MHz) para valorar la pared intestinal. Se ha intentado que los pacientes estuvieran en ayunas, aunque no siempre ha sido posible. En la mayoría de las ocasiones, la realización de la ecografía ha sido muy próxima en el tiempo a la de la entero-RM.
Intestino y mesenterio normales en ecografía:
• Las sondas con frecuencias entre 7,5 y 14 MHz permiten visualizar la estratificación normal de la pared intestinal, en la que se diferencian 5 capas:
◦ Interfase mucosa ecogénica.
◦ Mucosa hipoecoica.
◦ Submucosa hiperecoica.
◦ Muscularis propia hipoecoica. ◦ Serosa hiperecoica.
-
Grosor normal en niños:
◦ Pared de intestino delgado: < 2,5 mm.
◦ Pared de colon: < 2 mm.
◦ NOTA: un segmento intestinal con un grosor mural > 3 mm es patológico. -
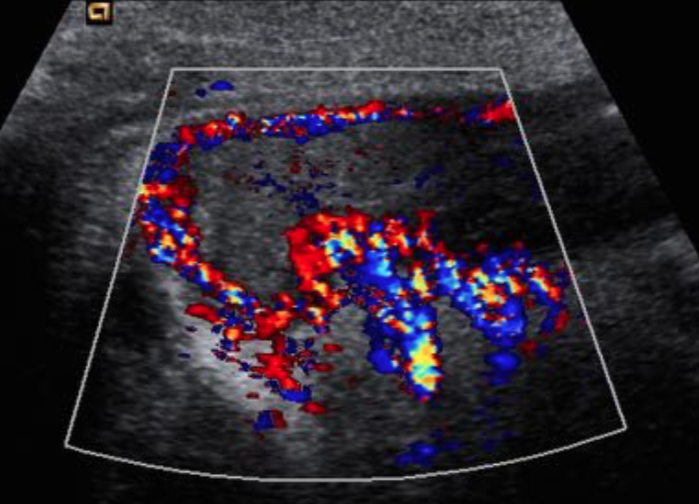
Doppler-color: el intestino normal no muestra vascularización o esta es muy escasa.
-
El intestino es compresible y peristáltico.
-
El yeyuno se diferencia del ileon porque contiene más pliegues; cuando las asas intestinales están
afectadas, es muy difícil diferenciar entre yeyuno e ileon.
-
El mesenterio se objetiva como múltiples estructuras ecogénicas paralelas aperistálticas, con
escasa vascularización.
Descargas
Citas
Hammer MR, Pobderesky DJ, Dillman JR. Multidetector Computed Tomographic and Magnetic Resonance Enterography in Children: State of the Art. Radiol Clin N Am 2013; 51: 615-636
Torregrosa A, Pallardó Y, Hinojosa J, Insa S, Molina R. Enterografía por resonancia magnética: técnica e indicaciones. Hallazgos en la enfermedad de Crohn. Radiología 2013; 55 (5): 422-430
Athanasakos A, Mazioti A, Economopoulos N, Kontopoulou Ch, Stathis G, Filippiadis D, Spyridopoulos T, Alexopoulou E. Inflammatory bowel disease — the role of cross-sectional imaging techniques in the investigation of the small bowell. Insights Imaging 2015; 6: 73-83
Biko DM, Rosenbaum DG, Anupindi SA. Ultrasound features of pediatric Crohn disease: a guide for case interpretation. Pediatr Radiol 2015; 45: 1557 - 1566
Ziech MLW, Hummel TZ, Smets AMJB, Nievelstein RAJ, Lavini C, Caan MWA et al. Accuracy of abdominal ultrasound and MRI for detection of Crohn disease and ulcerative colitis in children. Pediatr Radiol 2014; 44: 1370 - 1378
Mentzel H-J, Reinsch S, Kurzai M, Stenzel M. Magnetic resonance imaging in children and adolescents with chronic inflammatory bowel disease. World J Gastroenterol 2014; 20(5): 1180 - 1191
Dillman JR, Smith EA, Sanchez R, DiPietroMA, Dehkordy SF, Adler J et al. Prospective cohort of ultrasound-ultrasound and ultrasound-MR enterography agreement in the evaluation of pediatric small bowel Crohn disease. DOI 10.1007/s00247-015-3517-3
Maccioni F, Al Ansari N, Mazzamurro F, Civitelli F, Viola F, Cucchiara S, Catalano C. Detection of Crohn disease lesions of the small and large bowel in pediatric paients: diagnostic value of MR Enterography versus reference examinations. AJR 2014; 203: W533 - W542
Duigenan S, Gee MS. Imaging of pediatric patients with inflammatory bowel disease. AJR 2012; 199: 907 - 915
Smith EA, Dillman JR, Adler J, Dematos-Maillard VL, Strouse PJ. MR enterography of extraluminal manifestations of inflammatory bowel disease in children and adolescents: moving beyond the bowel wall. AJR 2012; 198: W38 - W45
Sohn B, Kim M-J, Koh H, Hwa Han K, Lee M-J. Intestinal lesions in pediatric Crohn disease: comparative detectability among pulse sequences at MR enterography. Pediatr Radiol 2014; 44: 821 - 830
Mollard BJ, Smith EA, Lai ME, Phan T, Christensen RE, Dillman JR. MR enterography under the age of 10 years: a single institutional experience. Pediatr Radiol 2016; 46: 43 - 49
Barkmeier DT, Dillman JR, Al-Hawary M, Heider A, Davenport MS, Smith EA, Adler J. MR enterography-histology comparison in resected pediatric small bowel Crohn disease strictures: can imaging predict fibrosis? Pediatr Radiol DOI 10.1007/s00247-015-3506-6
Ream JM, Dillman JR, Adler J, Khalatbari S, McHugh JB, Strouse PJ et al. MRI diffusion-weighted imaging (DWI) in pediatric small bowel Crohn disease: correlation with MRI findings of active bowel wall inflammation. Pediatr Radiol 2013; 43: 1077 - 1085
Neubauer H, Pabst T, Dick A, Machann W, Evangelista L, Wirth C et al. Small-bowel MRI in children and young adults with Crohn disease: retrospective head-to-head comparison of contrast-enhanced and diffusion-weighted MRI. Pediatr Radiol 2013; 43: 103 - 114
Dillman JR, Smith EA, Sanchez RJ, DiPietro MA, SeMatos-Maillard V, Strouse PJ, Darge K.Pediatric small bowel Crohn disease: correlation of US and MR Enterography. Radiographics 2015; 35: 835 - 848
Casciani E, De Vincentiis Ch, Polettini E, Masselli G, Di Nardo G, Civitelli F et al. Imaging of the small bowel: Crohn ́s disease in paediatric patients. World J Radiol 2014; 6(6): 313 - 328
Chiorean L, Schreiber-Dietrich D, Braden B, Cui X-W, Buchhorn R, Chang J-M, Dietrich Ch F. Ultrasonographic imaging of inflammatory bowel disease in pediatric patients. World J Gastroenterol 2015; 21(17): 5231 - 5341
Towbin AJ, Sullivan J, Denson LA, Wallihan DB, Podberesky DJ. CT and MR Enterography in children and adolescents with inflammatory bowel disease. Radiographics 2013; 33: 1843 - 1860
Quencer KB, Nimkin K, Mino-Kenudson M, Gee MS. Detecting active inflammation and fibrosis in pediatric Crohn ́s disease: prospective evaluation of MR-E and CT-E. Abdom Imaging 2013; 38: 705 - 713
Levine A, Koletzko S, Turner D, Escher JC, Cucchiara S, de Ridder L et al. ESPGHAN revised Porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. JPGN 214; 58(6): 795 - 806
Bosemani T, Ozturk A, Tekes A, Hemker MO, Huisman TAGM. Feasibility of an optimized MR enterography protocol in the evaluation of pediatric inflammatory bowel disease. JBR-BTR 2013; 96: 196 - 202
Spieler B, Hindman N, Levy J, Zabriesky K, Sahlein D, Seuss C, Kim S. Contrast-enhanced MR enterography as a stand-alone tool to evaluate Crohn ́s disease in a paediatric population. Clin Radiol 2013; 68: 1024 - 1030
Álvarez Beltran M, Barber Martinez de la Torre I, Segarra Cantón O, Redecillas Ferreiro S, Castellote Alonso A, Infante Pina D. Utilidad de la entero-resonancia magnética en el estudio de la enfermedad de Crohn pediátrica. An Pediatr (Barc). 2013; 78(5): 314 - 320
Shenoy-Bhangle AS, Nimkin K, Aranson TS, Gee MS. Value of diffusion-weighted imaging when added to magnetic resonance enterographic evaluation of Crohn disease in children. Pediatr Radiol 2016; 46: 34 - 42
Garcia Vilela E, de Gama Torres HO, Paiva Martins F, de Abreu Ferrari MdL, Menezes Andrade M, Sales da Cunha A. Evaluation of inflammatory activity in Crohn ́s disease and ulcerative colitis. World Gastroenterol 2012; 18(9): 872-881